The Speech Of Silences In Therapy

The first axiom of human communication, the one that says that “it is impossible not to communicate” (Watzlawick et. Al), gives a specific theoretical body to affirm that silences in therapy speak for themselves.
There are numerous opportunities in which silences make up certain gaps in the dialogue. Many people try to fill in those gaps with superficial and luxurious words to alleviate the anguish that underlies them.
In this sense, covering those gaps of silence avoids, as a defense, entering into anguish immediately, anguish as a result of the conflicts in which the person is involved. Let’s go deeper.

The meanings of silences
It would be impossible to make a classification of silences in therapy and in any type of relationship. Not only because of the great subjectivism that it supposes, but because it would depend on the relativity implied by the attribution that the interlocutor would encode.
Every time we perceive something, we make our own interpretation, within the possible thousands. This is because human beings live and interact by attributing categories to actions. And in gestural language is where greater emphasis is placed on projecting the attribution that is believed to be the most appropriate, than by not checking with the interlocutor, you run the risk of building a self-fulfilling prophecy.
Therefore, in any human dialogue, it is important not to stay in the categorization and try to metacommunicate avoiding the assumption through questions such as: what does this deep silence mean ?; what are you saying?; what are you talking about?
In interventions that have to do with non-verbal language, the instrumentation of silences at different moments of a relationship produces effects that engage any point of dialogue. For example, silence can be a restraining company, although it can also be provocative. It all depends on the section of the dialogue sequence and the impact on the experiences.
Whatever the reason that originated the silence, it is a propitious moment for the acute observation of all the non-verbal features of the other, such as the gestures of the face, the body posture and, mainly, the gaze. These signs allow, he asks by means of, to interpret the gestures more correctly and to inquire about it.
Types of silences in therapy
There are different times when silences occur in therapy. A keen observation of the patient’s attitudes can help to understand silence with different meanings.
Silences of boredom
For example, there are silences in boredom therapy. They are those that arise when a theme or problem is repeated and repeated, without finding an echo of a solution in the action.
The therapist not only gets bored with the usual speech, but it is the same patient who gets bored talking more about the same, with more of the same result. On many occasions, this silence is the result of the complaint. The patient complains, criticizes and ruminates, while immersing himself in inaction.
Silences of resistance and reflection
At other times, silences of resistance are observed, in which patients shy away from entering the work of the problem that afflicts them. They are silent while playing from the perimeter about what is happening to them and making banal comments … until the escape script concludes in the session, but not in their life.
The therapist may denounce this game in an untimely way or simply observe and smile wryly, in an attempt to generate the patient’s curious question about his attitude.
After a provocative or redefining intervention, a thinking, reflective silence is established. Then the patient mumbles the therapist’s point, associates and understands, or at least tries to think about what the therapist pointed out.
Silences of anguish
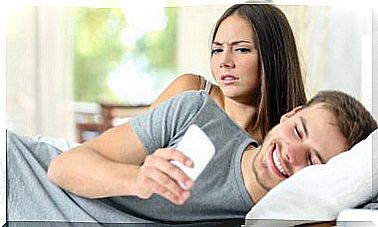
Many are the silences of anguish that arise in therapy. In general, they are the result of a conflictive situation that deeply affects the emotions and does not produce a verbal effect, but rather a silent cry. This type of silence can also arise in relation to a therapeutic intervention with a strong affective tenor.
In certain moments of escalation, in a couple or in a family, attaching a certain gesture of sadness to the therapist, silences can be a low blow. At times, they manage to end an aggressive style of interaction and plunge the members into a long, anguished silence. A man fixes his eyes on the floor. A lady shows her first tears. A boy covering his ears and a teenager looking out trying to swallow.
Silences of disinterest
There are also the silences in therapy of disinterest, or rather, of the lack of awareness of the importance of a problem or its existence. These are common in the person who attends therapy by decision of others, such as an adolescent who is sent by his parents, and in those who disbelieve in psychotherapy.
Silences of defiance and expectation
In therapy, silences of challenge may arise, in which the person attends the session, not only disbelieving in the effectiveness of a treatment, but also with the secret intention – as Watzlawick points out – to “defeat” the expert. This type of silence awaits the intervention of the therapist, with the secret expectation of confronting or denying it.
Unlike these, the silences of expectation do not seek to deny or confront the therapist. On the contrary, the patient has a remarkable desire to express what is happening to him, hastened to solve his problem, and for this very reason he pours out a gush of stories, phrases and anecdotes and then anxiously awaits the return of the therapist.
In these cases, the expectations placed on psychotherapy and on the word of the professional are very high. The person looks insistently at the professional, with his body hunched forward in his seat, waiting for an answer. Your body language says: You! what do you think about what happens to me doctor!
Silences of bewilderment and some others
The silences of confusion are those that are established in the face of an intervention that is unexpected, or that is unintelligible for the patient, or because it alters rational logic. These silences seek the answer in the therapist. The person shakes his head as if to say: It can’t be ..! I don’t understand … and he looks at the professional in an attitude of waiting to make the situation understandable.
Other silences transform anguish into anger. The person bites his cheeks, moves his jaw, contracts his fists, occasionally hits one fist with another, contracts. This type of silence is the result of connecting, among other things, with stories of pain, experiences of having been manipulated, unjust deaths, or provocative or ironic therapeutic interventions.
There are silences that simply show a telegram-like communication style. This is the type of silence of people who, in general, speak little and when they are about to tell a story, they do not go into details or accompanying anecdotes, they are, rather, guttural in their expressions. Many of them are shy or embarrassed or undervalued who believe they have little to contribute to the conversations.
Other times, silences have to do with attention, or respect for the interlocutor. A therapist speaks and the person is silent because he is attentive to what they are saying.
As we have already pointed out, some people have a telegram-like communication style, speak little and are listeners most of the time. But there are some who are only like this in therapy to show excessive respect for the word of the professional, but then they can be invasive and disqualifying with the rest of the people.
Take care in the interpretation of silence
It is important to be prudent in interpreting silence. A wrong categorization can lead to greater confusion in the relationship with our interlocutors.